
Gray scale trans abdominal longitudinal view Ultrasonography of uterus in a 34 year old female showing multiple an-echoic areas within the myometrum of the anterior wall (arrow) displacing the thin linier endometrium (arrow head).

On colour Doppler there are multiple colour filled dilated vascular channels.
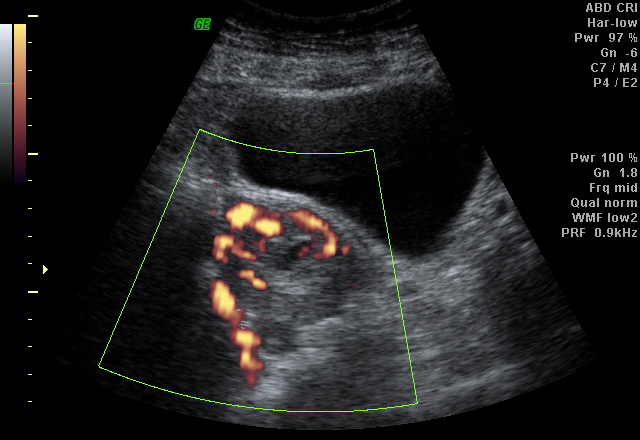
Power Doppler depicting the color flow within the lesion

Spectral wave form at the feeding artery showing high velocity and relatively high resistant arterial flow.

Spectral tracing in the draining vein showing venous flow. The findings are consistent with uterine arteriovenous fistula. Patient had history of recent medical termination of pregnancy with dilatation of curettage.
Discussion:
Uterine vascular malformations include:
- Arteriovenous malformations (AVM) (especially arteriovenous fistulas).
- True aneurysms.
- Pseudoaneurysms.
It is otherwise called with several terms which are cavernous hemangioma, cirsoid aneurysm, racemose aneurysm, arteriovenous aneurysm, pulsatile angioma, and arteriovenous fistula.
Etiology:
AV fistulas are usually acquired and typically represent a single artery joining a single vein.
They result as a consequence of previous uterine trauma (eg, prior pelvic surgery, curettage), use of intrauterine contraceptive devices, pathologic pregnancy-related events, and previous treatment for gestational trophoblastic disease.
Clinical Features:
Vaginal bleeding- Most common.
Congestive heart failure - secondary to steal phenomenon - Less common.
Imaging findings:
USG:
- Gray-scale US shows a normal-appearing endometrium, whereas the myometrium contains multiple hypoechoic or anechoic spaces.
- At color Doppler US, these cystic spaces generate color signals in a mosaic pattern representing turbulent flow.
- Spectral analysis of the arterial vessels within the lesion shows high-velocity flow with a low resistive index (approximately 0.51–0.65). Spectral analysis of venous flow demonstrates a similar pattern.
CT: CT angiography of the pelvic vessels may reveal the vascular malformation.
MRI:
Multiple dilated tubular channels showing flow related signal voids (hypointense) on T1 and T2 images seen in myometrium with normal endometrium or displaced endometrium. The flow relted signal void channels may or may not extend in to the parametrium.
Treatment:
MRI:
Multiple dilated tubular channels showing flow related signal voids (hypointense) on T1 and T2 images seen in myometrium with normal endometrium or displaced endometrium. The flow relted signal void channels may or may not extend in to the parametrium.
Treatment:
- Acute treatment - Hemodynamic stabilization and management of active bleeding.
- Occlusion with a Foley catheter bulb may be effective.
- If fertility is not an issue, hysterectomy is the treatment of choice
- They may be treated successfully with intra-arterial embolization
*******

No comments:
Post a Comment