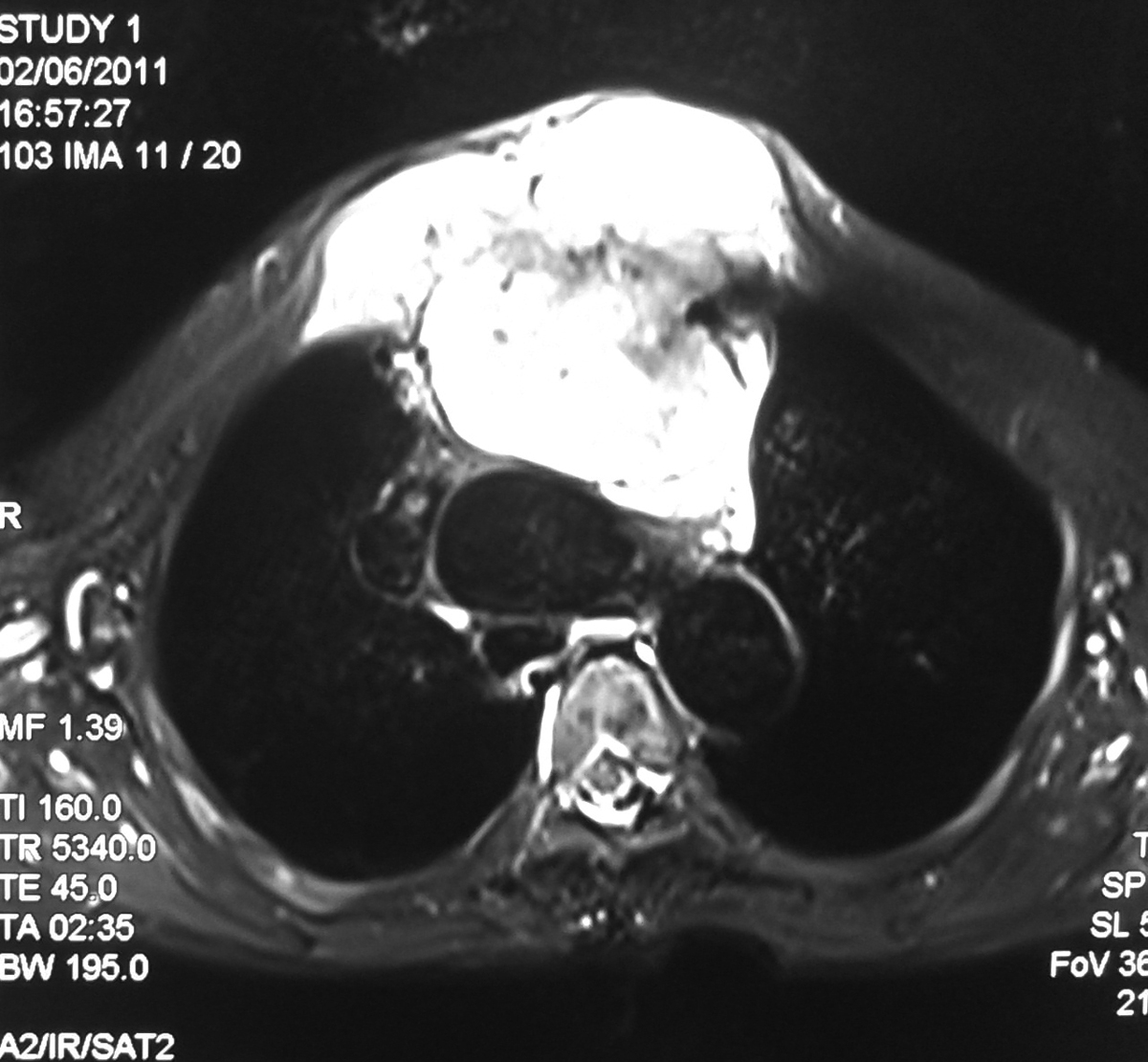
32 Year old male with road traffic accident showing posterior dislocation of the elbow joint with mild proximal migration of the radius and ulna and small displaced chip fracture of the coronoid process.

MRI sagittal T2 images showing posterior dislocated elbow.
Discussion:
- Elbow dislocation is the second most common major joint dislocation.
- Dislocation is usually closed and posterior.
- Dislocations of elbow usually result from fall onto extended elbow.
- Anatomic morphology of semilunar notch may predispose to elbow dislocation.
- Central angle of semilunar notch is significantly larger in group of pts who had dislocation of the elbow compared to normals.
- Classified according to direction of dislocation, namely posterior, posterolateral, posteromedial, lateral, medial, or divergent.
- Simple - elbow dislocations without fracture.
- Complex - dislocations with fracture.
- Rupture of capsule, rupture of MCL, lateral ligaments, rupture of flexor pronator mass and less commonly, injury to brachialis muscle.
- Rupture of brachial artery has been reported.
- Dislocation with radial head fracture is most common complex dislocation as in our case.
- Fracture dislocation with MCL injury: radial head fracture & MCL Instability:
- Terrible Triad: (dislocation, cornoid process #, and radial head #).
Neurologic injury:
- Compartement syndrome.
- Neuropraxia.
- Ulnar nerve injury in 14%.
- Entrapment of median nerve.