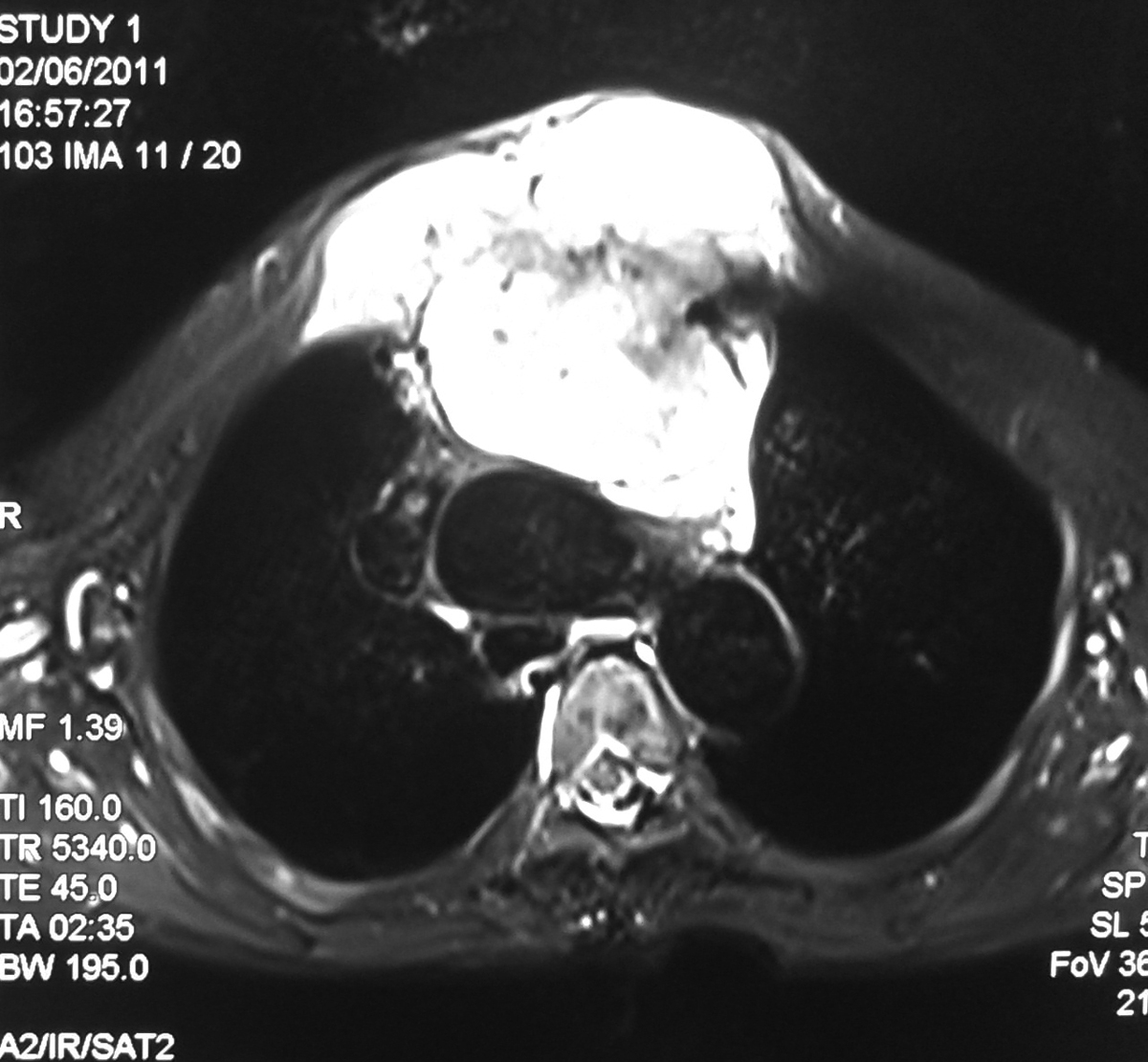
45 year old male with history of high grade fever and foul smelling expectorations. Chest radiograph showed well defined thick walled cavitory lesion in the right lower lobe with air fluid levels consistent with lung abscess.
Discussion:
A primary abscess is one which develops as a result of primary infection of the lung. They most commonly arise from aspiration, necrotising pneumonia or chronic pneumonia, e.g. pulmonary TB
A secondary abscess is one which develops as a result of another condition. e.g: bronchial obstruction: bronchogenic carcinoma, inhaled foreign body.
Plain Radiograph: The classical appearance is a cavity containing an air-fluid level. In general abscesses are round in shape, and appear similar in both frontal and lateral projections. Additionally all margins are equally well seen, although adjacent consolidation may make assessment of this difficult.
CT scan:
CT is the most sensitive and specific imaging modality to diagnose a lung abscess. Abscesses vary in size, and are generally rounded in shape. The may contain only fluid or have an air-fluid level. Typically there is surrounding consolidation, although with treatment the cavity will persist longer than consolidation.
The wall of the abscess is typically thick and the luminal surface irregular.
Treatment and prognosis:
Lung abscesses are usually managed with prolonged antibiotics and physiotherapy with postural drainage.
Complications
Complications of surgery or percutaneous drainage include :
Empyema
Bronchopleural fistula
Haemorrhage (from chest wall or from lung).
CT is the most sensitive and specific imaging modality to diagnose a lung abscess. Abscesses vary in size, and are generally rounded in shape. The may contain only fluid or have an air-fluid level. Typically there is surrounding consolidation, although with treatment the cavity will persist longer than consolidation.
The wall of the abscess is typically thick and the luminal surface irregular.
Treatment and prognosis:
Lung abscesses are usually managed with prolonged antibiotics and physiotherapy with postural drainage.
Complications
Complications of surgery or percutaneous drainage include :
Empyema
Bronchopleural fistula
Haemorrhage (from chest wall or from lung).