
Axial CT section through the optic nerves in a 59 year old male with trauma showing fracture in the posterior part of the lateral wall of the right orbit and the fracture fragment is causing compression on the optic nerve at the optic canal (arrow) and note the normal wide optic canal on left side (arrow head).

Coronal CT scan bone window showing the bony fragment compressing the optic nerve and narrowing the optic foramen (arrow) and note the normal foramen on left side (arrow head).

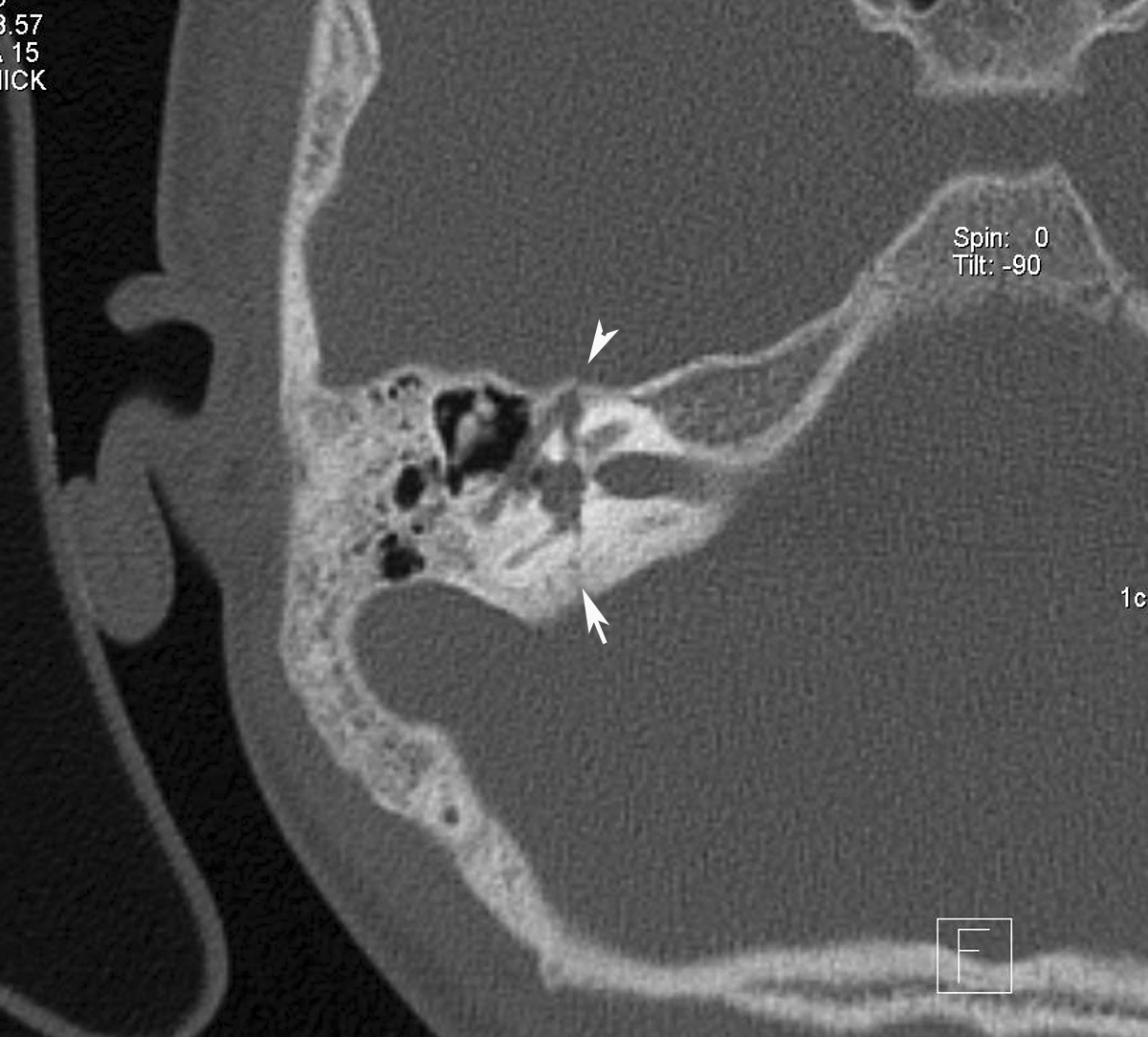
Sagittal image showing the bony fragment compressing on the optic nerve.
Discussion:- Traumatic optic neuropathy is a devastating potential complication of closed head injury.
- The hallmark of an optic neuropathy, traumatic or otherwise, is a loss of visual function, which can manifest by subnormal visual acuity, visual field loss, or color vision dysfunction.
- Vision loss associated with traumatic optic neuropathy can be partial or complete and temporary or permanent.
- Best diagnostic test is Thin-slice CT scan of the nose, sinuses, and orbits
- Fractures through the optic canal can be best depicted with thin-section CT scanning (eg, 1.5-mm cuts with 1-mm intervals).
- CT scanning provides adequate imaging of orbital soft tissue and is better than MRI at delineating bony defects.
- It provides an intraoperative road map for the surgeon in patients who require surgical decompression and can be used for image guided endoscopic surgery.
- Treatment is observation, steroids and optic nerve decompression. The decision for surgical decompression should still be based primarily on the clinical examination findings.











{kind=link}